Thoughts on Mild Traumatic Brain Injury Rehab
Mild Traumatic Brain Injury Rehab must start with recognition that long term deficits could persist after a seemingly transient event. While excellent treatment options exist, treatment systems are not set up to get the survivor to the proper rehab professionals.
By Rebecca Martin
In previous blogs we have discussed some of the short term and long term symptoms of acquired brain injury and more specifically, the propensity for those symptoms to lead to psychological issues down the road. In the medical environment those with more severe symptoms are more likely to receive the attention and treatment to endeavor to facilitate a return to pre-injury life successfully. However, mild brain injuries often come with long term deficits which are often not addressed by the medical community. It is not uncommon to get lost in the system with dire consequences for the patient.
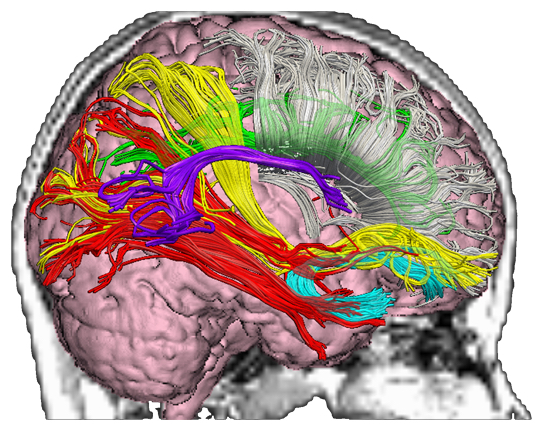
Mild traumatic brain injury rehabilitation is critical for better outcomes but our primary care based medical referral system does not accommodate treatment for something deemed temporary in the acute stage of the injury. What makes recovery difficult is that the primary injury is to axonal tracts, as shown above, not to the larger macroscopic structures of the brain.
The most common symptoms which manifest both in the short term and the long term are those that affect cognitive skills. We will be looking at these issues as they pertain to what is referred to as mild traumatic brain injury with an emphasis that the word mild does not describe the potential for devastating deficits long term.
Cognitive Functions Disrupted after MTBI
Cognitive functions embody attention, memory and executive functioning and can further be broken down into more distinct disturbances. First is the overall cognitive ability. Attention is a component that can be further looked at in terms of selective attention, inhibition control, and divided attention. Perhaps this is better understood by looking at an individual’s ability to focus on a task at hand, or to focus on multiple tasks, the ability to focus in the presence of distractions, and more importantly, absorb the information presented through appropriate focus.
Domains that Need Attention in Mild Traumatic Brain Injury Rehab
Attention is often described in four components; working memory, competitive selection, top-down sensitivity control and filtering for stimuli. Working memory is the ability to remember the amount of information to complete a task. This is not to be confused with long term memory which involves a lifetime of information. An example might be remembering a grocery list or any of the short term details it takes to complete a cognitive task. Competitive attention selection occurs when we filter out stimuli which are non-essential to the task at hand in order to focus on those stimuli which are essential to complete the task at hand.
Editors Note: While carbon monoxide brain damage is often considered a different type of brain damage than Mild Traumatic Brain Injury, the deficits therefrom and the needs for rehabilitation from it are very similar to that of MTBI. For our treatment of brain damage from carbon monoxide poisoning, click here.
Top-down and bottom- up attention are concepts referring to the way we prioritize stimuli. Top-down refers to the way we intentionally focus on the stimuli presented to us. We can focus on the dialogue in a movie without being distracted by the background music or other ambient noise in order to follow a plot. Bottom-up attention would be if the other stimuli automatically take the attention even if we had no intention of allowing it to do so thus impairing our ability to follow the plot. The difference here is our intention to focus on certain stimuli in the presence of other stimuli. The latter is synonymous with filtering for stimuli.
Memory Needs Focus in Mild Traumatic Brain Injury Rehab
Memory can be similarly broken down into several components. We have incidental memory, immediate memory, learning memory, and delayed recall. Incidental memory is non-intentional and involves remembering things one was not asked to remember, especially in a learning environment. We may learn a new skill in a fun and interesting way without realizing that activity has improved a more important skill such as hand/eye coordination. Playing games is one way we learn incidentally.
Intentional learning is when we, with purpose, set out to memorize certain materials in an effortful way. In this case, our purpose and intention is to acquire that knowledge.
Learning memory is what we consider that memory that allows us to acquire a skill or knowledge and to express what we have learned.
Delayed recall not only includes our ability to recall information at a later time but also our ability to recognize familiar information or information we have already learned. All of these memory issues must be addressed in mild traumatic brain injury rehab.
Executive Functioning Deficits Perhaps Most Debilitating
Other parts of executive functioning include adaptable thinking, planning, self-monitoring and time management. Disruptions in executive functioning may make it difficult to start and complete tasks, to control our emotions and impulses and can also result in inappropriate social behavior.
Many studies have been done suggesting that impairments in many of these functions are common in those following a mild traumatic brain injury. And that these can occur in the acute stage immediately following an injury and in the long term and the numbers of those impacted are significant.
In the preface to a report from the National Center for Injury Prevention and Control. Report to Congress on Mild Traumatic Brain Injury in the United States: Steps to Prevent a Serious Public Health Problem. Atlanta, GA: Centers for Disease Control and Prevention; 2003. it is stated that:
“In recent decades, public health and health care communities have become increasingly aware that the consequences of mild traumatic brain injury (MTBI) may not, in fact, be mild. Epidemiologic research has identified MTBI as a public health problem of large magnitude, while clinical research has provided evidence that these injuries can cause serious, lasting problems.”
Cognitive Rehabilitation Therapy for MTBI
The rehabilitation process for cognitive deficits is called Cognitive Rehabilitation Therapy (CRT). Unlike physical deficits following an injury, CRT is often not covered by insurance. CRT is not considered a psychological methodology like cognitive behavioral therapy which addresses psychiatric concerns. However there are means to challenge the insurance on the necessity of the treatment, usually enlisting the cooperation of families and providers.
CRT is made up of two different treatments; restorative and compensatory. The first is designed to improve the cognitive system and the second to compensate for the deficits.
Mild Traumatic Brain Injury Treatment Specialists
There is a wide variety of providers for such services; speech pathologists, occupational and physical therapists, neuropsychologists, counselors in vocational rehabilitation, and physiatrists. Nursing staff may also be used depending on the specific details of the deficits. Most programs are specifically designed for the particular problems a patient is having. Treatment may occur in the hospital, inpatient or outpatient, or in rehabilitation facilities. But if you are not hospitalized at the time of injury, referral to CRT services is unlikely. This is because most emergency rooms are not reporting on cognitive issues at the time a patient is seen and the patient often does not realize the extent of their cognitive issues until they return to school or work. In fact, 90% of patients who find themselves in an emergency room with a mild brain injury have a negative CT scan because the imaging technique is not sensitive enough to detect the type of damage indicative of a mild brain injury.
Often the patient is reluctant to seek medical help for the difficulties they experience after an injury. They were one person before injury and seem to be another person after the injury but because of cognitive disruptions, the correlation between the injury and the issues may not be an automatic assumption on the part of the patient. The classic way to assess the cognitive disruptions, in the absence of neurological evidence, is through the use of a neuropsychologist who can administer standardized tests to determine where the deficits are.
Attention Processing Training is used to help improve disruptions in attention functioning and has shown promise in improving the ability to focus over the course of several weeks. Time is of the essence as the longer deficits are in place, the greater the chance that depression and anxiety can occur and hamper efforts at rehabilitation.
Therapists can assist with setting goals, and keeping patients on track and managing aspects of daily living. Schedules may need to be adjusted to compensate for the fatigue an injured brain may experience returning to normal tasks. Taking more breaks may be a necessity. Physical health can play a role by increasing the energy levels needed to compensate for the fatigue. It should be noted that drugs and alcohol should be avoided as they slow recovery and escalate the chance of another injury.
There are some things an individual should consider after a mild brain injury. One is keeping a journal of what deficits they are experiencing on a daily basis. This information is invaluable when seeking help to focus in on what is the most detrimental to one’s previous level of functioning. The other is, in essence, some form of day planner to help with setting and achieving goals, following through with treatment, and relieving the burden on a damaged brain struggling to keep up. There is a great checklist at https://www.headway.org.uk/about-brain-injury/individuals/brain-injury-and-me/9-ways-to-help-with-planning-problems-after-brain-injury/
It is important to remember the many consequences of impaired cognitive functioning in any discussion of the deficits. Frustration, fatigue, and isolation can often be the result. Behavior can be affected which the person suffering from a mild brain injury might be oblivious too, only perceiving the changed reactions of those around them. Relationships may suffer as a result. Headway, a brain injury association, recommends this checklist for an open discussion with a loved one who is having difficulty identifying that there might be an ongoing issue https://www.headway.org.uk/about-brain-injury/individuals/effects-of-brain-injury/executive-dysfunction/
How does one start the treatment process after a mild brain injury if no treatment has been forthcoming? One can go to their general practitioner or primary care doctor and request a referral to a neuropsychologist for testing. Neuropsychological testing is not pass or fail, it is designed to identify the areas of the brain and its functioning which are impaired. In this way they can help determine what types of intervention would be the most helpful, something which cannot be provided by imaging alone. Once problems in functioning are identified, personalized treatment can be recommended to help address the deficits or to determine what type of compensatory aids might be the most beneficial. According to the Headway booklet:
“Rehabilitation of executive dysfunction can be challenging and requires an individualized approach to treatment. The rehabilitation programme for each patient will depend on their goals, the nature of their difficulties, self-awareness, readiness to engage in treatment, level of social support and presence of other issues such as mood disturbances.”
It is also recommended that caffeine intake is reduced after a mild brain injury and this includes over the counter medications which contain caffeine such as Excedrin and Anacin. Disturbed sleep patterns contribute to the frustration, irritability and fatigue experienced after a mild brain injury. Medical intervention may be needed to re-establish normal sleep patterns.
In general it is a holistic approach when discussing rehabilitation for mild brain injury. Education is a key ingredient to outcome. If the patient is not absolutely aware of the scope of the changes in mood and personality, then it is up to the family to become as educated as possible to the nature of the symptoms and the interconnectivity of the separate medical and therapy resources. Each individual’s treatment will be different depending on the areas of the brain impacted, age, previous history of brain injury, education level and other factors. All of these things need to be taken into consideration when designing a program of care. The only thing we can be confident about is that delaying or ignoring the issues can ultimately lead to mental distress such as depression and anxiety and even worse outcomes. We spoke previously about the heightened risk of suicide in mild brain injury and especially, untreated mild brain injury. And we spoke candidly about how quickly a school age person might develop the type of depression to be concerned about in a very short period of time compared to an adult.
Though you will encounter numerous medical professionals insisting that taking a couple of aspirin and getting some rest as a cure all for mild brain injury, modern research is proving again and again that not all are that fortunate and long term deficits are finally being understood as more of a crises they can become on a far larger scale than previously thought. The best solution is more immediate and appropriate care from the onset. Even so, some deficits may be improved while others may require a permanent compensatory strategy.
Other Neurological Deficits after MTBI
One of the symptoms of mild brain injury is damage to the oculomotor system, which impacts our ability to track objects in an environment and our reaction time to them. This can impact everything from our ability to read to our ability to drive.
Studies have concluded that this may be one long term symptom of even a mild brain injury. Danna-Dos-Santos, A., Mohapatra, S., Santos, M. et al. Long-term effects of mild traumatic brain injuries to oculomotor tracking performances and reaction times to simple environmental stimuli. Sci Rep 8, 4583 (2018). https://doi.org/10.1038/s41598-018-22825-5 They concluded that:
“Results indicated the presence of impairments to basic neural functions used to explore and respond to environmental demands long after the occurrence of mTBIs.”
This may be experienced as nausea or dizziness as well and should be brought to the attention of a physician for safety purposes. In the case of patients who depend on visual cues for the safe performance of their jobs this is something that should be addressed prior to returning to the job. As in the case of any significant deficit which can impact job performance, it may be necessary to seek out vocational rehab as well. In an article entitled Vocational Rehabilitation in Mild Traumatic Brain Injury: Supporting Return to Work and Daily Life Functioning https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6393356/ they found:
“Persisting symptoms may delay return-to-work (RTW), reduce work productivity, adversely affect quality of life, and result in additional social and economic costs.”
In some cases, a partial return to work is suggested following a mild brain injury rather than diving back into one’s former routine head first.
Though it is not a pleasant thought that the short term effects of a mild brain injury might continue indefinitely, more and more research is helping us understand the mechanics of these types of injuries and strategies are evolving to improve or provide compensatory skills to alleviate some of the hardships that can be encountered. However, as I have encountered in my research, there is no fast and easy solution and it is often a multi-disciplinary approach which provides the best results.
For more information about options for mild traumatic brain injury rehab go to https://www.biausa.org The Brain Injury Association of America, along with your local state brain injury associations, can provide an essential starting point.
The Brain Injury Law Group has been publishing information about MTBI for 25 years, with it being the primary focus of http://tbilaw.com published in 1996. Our most comprehensive treatment of this subject is at https://braininjuryhelp.com/mild-traumatic-brain-injury See also https://braininjuryhelp.com/sitemap/ for a comprehensive table of contents of our brain injury information.


I want to know more.